Terms of reference On March 16, 2022, Honourable Mike Farnworth {
needs to be added to @Glenn's most despised list - and he "announced" the 'appointments' of this review}, Minister of Public Safety and Solicitor General, announced the appointment of an independent project team made up of the three of us—Bob de Faye, Dan Perrin, and Chris Trumpy—to conduct a review of the British Columbia public sector’s response to the COVID-19 pandemic. The full terms of reference of the review are
attached as Appendix A. The objective of this review is to learn from the COVID-19 experience and to apply those learnings to be better prepared for the province-wide emergency. To do so, we have been asked to conduct an operational review of government’s response. The document specifically
excludes “
an assessment of economic recovery and public policy decisions made by government to deal with the consequences of the pandemic and decisions made by the independent Provincial Health Officer”
from the scope of the review. That exclusion received
a certain amount of criticism when the review was announced. Not reviewing the decisions themselves allowed our team and those we spoke with to focus on
operational matters—how the large machine of government was able to adjust and respond {"operational matters" indeed. Who needs an economy}. Nevertheless,
criticism the mandate received may in itself have reduced the number of organizations willing to engage with us {
thus no more criticism allowed in the future}. The reason why the decisions themselves were excluded from the scope was because
the next event will differ substantially from this pandemic, and the specific decisions made then will be informed by the circumstances at the time. Our mandate is to consider how the public policy decisions were made, communicated, and implemented. We also examine how government operations were adjusted in response to the pandemic. Those topics are covered in this report.
{
see Appendix A - it can't be copied and pasted}
Government 101 BC government’s pandemic response is a continuing all-of-government response that is extremely complex, involving almost all of the broad public sector and utilizing almost all of the mechanisms that government has at its disposal to deliver services and affect society. Our task is to undertake an operational review of this immense entity, with over 30,000 public service employees and about 500,000 public sector employees. As context to our review, the following provides an overview of what government does, how it is organized, and how it works, which we refer to as “Government 101.” {
one thing noticed in the press during "the operation," was the focus on the 30,000, however not a focus on the additional 500,000, and then add the service providers (private) who were all mandated, that is over a million people under their direct vaccine mandate control - many in the private sector and pretty much all unions would follow suite}
[...]
The types of public health tools used in response to a pandemic respiratory illness like the current pandemic focus on managing the likelihood of transmission of infection. They include both measures implemented by individuals changing their behaviour and measures taken by public health authorities. Not all of the tools listed were used in B.C. during the pandemic. The list is presented
in no particular order:
• hand washing and covering coughs and sneezes {
common sense}
• use of facemasks {
which originally the PHO dismissed, and then doubled down}
• cleaning and disinfection
• physical screens and barriers {
more items to clean}
• enhanced ventilation
• physical distancing
• reduced contacts
• identification of essential services {
liquor and cannabis stores where important, play grounds, no, not at all}
• gathering limits, event cancellations, and facility closures {
societal closure}
• capacity limits
• testing for infection management and surveillance purposes {
PCR 
}
• isolation when ill, whether self-isolation
or ordered quarantine
• case and contact management {
PCR and scary graphs}
•
lockdowns,
stay-at-home orders,
curfews,
and travel restrictions,
including border closures
• therapeutic medications and treatments {
many specialists were closed (locked down), and important or life saving treatments deferred}
•
vaccinations {
 they had such fun doing this to people, ruining their lives, their families and friends; very profitable coup de grace
they had such fun doing this to people, ruining their lives, their families and friends; very profitable coup de grace}
• requirements for
workers to be vaccinated
• limits on activities for those not vaccinated (
vaccine card or passport) {
another coup de grace}
All except vaccines and medications are referred to as non-pharmaceutical interventions and are typically intended to create stronger, but not fail-safe, layered protection. Several of these approaches were used concurrently in B.C. during the COVID-19 pandemic.
[...]
Alternatively, the Provincial Health Officer can, by
legal order, require people and businesses to comply with restrictions, including
not allowing some business to open, requiring others to reduce capacity, imposing mask mandates in certain public places, setting up contact tracing, and requiring people who have the virus or have been exposed to quarantine, and so on.
How are decisions made about what measures to take and the specific design details of the measure? In general,
the intention is to impose the fewest restrictions necessary at any given time for the
shortest period of time. A key principle underlying public health is doing
the least harm overall, including considering the harm caused by the disease together with the economic and the social effects of restricting activities {
note again, the terms of reference do not address the socioeconomic}
Science informs public health decisions
but does not dictate the decisions. It may be useful to briefly discuss
what science is and is not. Some perceive science to be a set of immutable facts that explain what we know of the world and beyond. In fact, science is a process (the scientific method) that provides a rigorous approach to continuously learning. Science generates knowledge that can be used in practice to guide areas like health care,
but very little in science is absolute or fully determined. As new knowledge is developed and tested, it creates new questions, often about ideas that many have taken for granted. In the case of the COVID-19 pandemic, since the SARS-COV-2 virus
had not previously been seen in humans, very little was known about it. Over the past two years, scientific knowledge about the virus and its variants has multiplied at a tremendous rate and will continue to grow. And, as a result, the best practices based on today’s knowledge may change quickly and significantly as knowledge grows and, of course,
as the virus evolves. Further, science cannot drive public policy decisions alone. Scientific evidence is very helpful in assessing the risks and harms associated with a disease and the effectiveness of the available public health measures. But other important considerations,
like social and economic implications of public health measures {
which they ae not suppose to mention as per the TR}, as well as their health effects for different groups within the population, all bear on the choice of measures put in place at a given time. In B.C., the COVID-19
Ethical Decision-Making Framework describes the process and considerations for making public health emergency response decision-making {
yes, ethics, cannot forget that - Oops}.
Circumstances constantly change during a pandemic. Scientific knowledge about the disease changes, sometimes very quickly, requiring guidance and orders to change. The disease itself changes as it evolves and as waves come and go. Treatments and
vaccines affect the level of risk {
so they say, yet mRNA risky would be an understatment} People’s behaviours and reactions to public health measures change. All these things affect what public health tools are used and the details of their design and implementation. Inevitably, public health emergency response decisions are complex, high-stakes judgment calls informed by
available information {
suppressed or otherwise}, which will change as circumstances change. Some of these decisions must be taken quickly and with
incomplete information, even when the public demands certainty and consistency to help allay their fears.
") ) and they should ask more questions of him ('Mr. Prime Minister, I'm just 6 and my friends and I are being told by you that we need covid mRNA vaccination when science tells us that we are not even at risk of covid and the shots have associated high dangers, why? and oh, one more question, do you force your own children to wear masks as we did for two years? and why would your do that to your children when masks are known to be dangerous?') . Of course, Justin then moved away form the core question/issue asked, and goes on about not everyone will agree, as leaders must make
) and they should ask more questions of him ('Mr. Prime Minister, I'm just 6 and my friends and I are being told by you that we need covid mRNA vaccination when science tells us that we are not even at risk of covid and the shots have associated high dangers, why? and oh, one more question, do you force your own children to wear masks as we did for two years? and why would your do that to your children when masks are known to be dangerous?') . Of course, Justin then moved away form the core question/issue asked, and goes on about not everyone will agree, as leaders must make 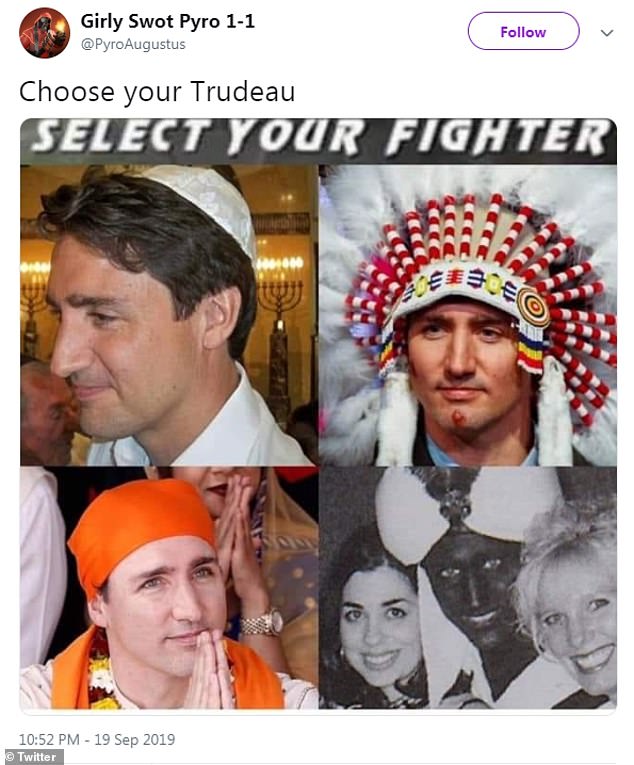
 verbalizing a fantastic simple observation
verbalizing a fantastic simple observation 



 }, the B.C. government and broader public sector, First Nations and Indigenous organizations {
}, the B.C. government and broader public sector, First Nations and Indigenous organizations { }
}
 } and the first doses of the vaccine arrived in B.C. a week later.
} and the first doses of the vaccine arrived in B.C. a week later. } movement grew through fall 2021, resulting in a weekslong occupation and disruption of downtown Ottawa starting January 2022, and continued with significant protests in Victoria’s Legislative Precinct in March 2022. When it seemed that the Delta wave was slowing down in December 2021, a public health order relaxed restrictions on bars, clubs, and restaurants on December 12 in time for the Christmas season and New Year’s Eve. However, the virus did not co-operate {
} movement grew through fall 2021, resulting in a weekslong occupation and disruption of downtown Ottawa starting January 2022, and continued with significant protests in Victoria’s Legislative Precinct in March 2022. When it seemed that the Delta wave was slowing down in December 2021, a public health order relaxed restrictions on bars, clubs, and restaurants on December 12 in time for the Christmas season and New Year’s Eve. However, the virus did not co-operate {