Rosemary Frei, MSc
August 27, 2022
A pharmacist named Jason Newman threatened me earlier this month.
Newman runs an organization called
FRAEM -- ‘The Foundation for the Responsible Administration of Emergency Medicines.’ It distributes large numbers of naloxone kits to members of the general public at places such as street festivals. I’d first encountered the organization in late June 2022 at a booth in downtown Toronto during the city’s Pride festival.
Naloxone is an opioid-overdose-reversing medication that’s usually used in
intranasal-spray or intramuscular-injection forms, as part of
‘take-home kits.’
After looking into FRAEM a little bit at the end of July 2022, I’d decided to try to find out more about that organization, Newman and naloxone. Newman keeps his name out of the public eye by not having his name on the FRAEM website or handouts. I tried to reach him by phone via the
number on the home page of the website but he didn't return my calls.
I’d therefore decided to visit
his pharmacy – which is has the same street address in the town of Delaware, Ontario, as an
organization FRAEM – in the hope that Newman would be there and talk to me. I arrived at the pharmacy -- on a short side trip while visiting my home town of London, which is just a few kilometres east of Delaware – on August 6 at 12:15 p.m., shortly before the pharmacy closed for the day. But the staff said he wasn’t in; they told me he was out of town.
I was hungry and ate lunch nearby. During the meal a friend of mine I was with decided to do an internet search for Newman’s name. I hadn’t done that yet.
Her quick search revealed that
Newman had been reprimanded for professional misconduct because of work he does via FRAEM -- that is, handing out naloxone to members of the public, door to door and in other venues such as street festivals, outside of his pharmacy and sometimes with and by associates of his who aren’t pharmacists. (See
this news report, and
this one,
this one,
this one, and the
early-2020 Ontario College of Pharmacists’ ruling against Newman. And
here is the Ontario College of Pharmacists’ guideline on dispensing naloxone.)
Therefore after lunch I decided to walk the short distance back to the pharmacy building and take a couple of photos of it from near the road, in case I later decided I wanted to include a picture of the pharmacy in a future article on naloxone. Here's one of my photos of it:
I was stunned when suddenly, a light-blue pickup truck pulled up beside me. The driver’s door opened. A man – who I realized must be Newman – gruffly told me to stop taking pictures, and that he wouldn’t answer my questions.
He ordered me to leave immediately and threatened to contact the cops and lawyers if I returned and took more photos. He called over to the driver of a car that was parked on the other side of me but who I couldn’t see. Newman was clearly signaling to me that it wasn't just him present and keeping an eye on me.
I left, waving goodbye to Newman and that unseen associate of his.
That situation was startling and scary. But it propelled me to probe beneath the glowing superficial image of the necessity for mass distribution of naloxone in the name of saving lives. (I also emailed the Ontario College of Pharmacists to let them know what had happened.)
What I've uncovered suggests that Newman’s actions are emblematic of the Wild West that surrounds naloxone being sold and dispensed to many millions of people -- usually without a prescription, with very little training and likely even less oversight -- in many countries.
Here’s a brief snapshot of the situation.
The kits are for use if someone sees another person who is unconscious from an opioid overdose. The people who have kits today include potentially a large number of
high-school students, and tens of millions of others who are given the kits via outlets such as
pharmacies, local public-health groups and community-based organizations.
Naloxone is also distributed to a very large number of
police officers,
other first responders, and people associated with religious organizations, and substance-use-recovery facilities,
school nurses, among many others. Moreover, most insurance plans in the US cover naloxone, which is also
frequently co-dispensed to people taking prescription opioids.
Those same people, in turn -- the majority of whom have no medical background -- follow what they’ve been told to do and spray or inject the naloxone into virtually every unconscious people they may come across, usually after just a few seconds’ cursory assessment of them.
Anyone who administers the drug is free from liability for injury or death of the person they give it to. This is thanks to such things as a ‘
standing order’ and ‘
Good Samaritan drug overdose’ laws. Governments, the manufacturers, pharmacists and all other individuals, companies and organizations that are involved in the wide dissemination of naloxone are all also exempt from responsibility, as far as I can determine.
From what I've been able to glean,
about 10-20% of the kits are used. And the majority of these are at safe-injection sites, where staff very frequently use the kits, to reverse overdoses of clients of the sites. The kits have expiry dates
18 to 24 months after manufacture, and therefore are restocked very frequently. (But researchers have found these expiry dates likely are "
grossly exaggerated" and are much shorter than they need to be.)
It turns out to be a big and multifaceted story. And as always, it’s instructive to follow the money.
There is a huge, lucrative and very fast-growing market for naloxone. One company is central in that market, but there are many other companies, organizations and individuals that are positioned to take a cut.
I’ve detailed my five main findings below, numbered 1 through 5.
Here’s a summary (clicking on each numbered paragraph brings you to the respective section):
1) An American company called Emergent BioSolutions dominates the sales of naloxone to governments. Emergent is continuing it's long-standing practice of using its oversized influence -- via, among other things, highly-placed lobbyists and a resolving door between powerful politicians and bureaucrats and Emergent’s executives and board members -- to make billions of dollars of sales for medical products that haven’t been objectively proven to be necessary or efficacious for protecting the public’s health.
2) Naloxone is associated with possible severe consequences such as heart attacks, strokes and death.
3) Accidental opioid-overdose death tallies likely are highly inflated. (I have four sets of supporting evidence -- 3A through 3D -- on this key point.)
4) There’s a financial incentive for pharmacists, and others, to distribute a lot of naloxone and to skirt regulatory bodies' guidelines in doing so.
5) Serious drawbacks of wide and indiscriminate naloxone dissemination occasionally come to the public’s attention – including solid evidence that it does more harm than good. However, that information quickly disappears from view under a wall of silence and/or criticism
Here is the detailed evidence supporting each of those points.
1. A very well-connected American pharma company called Emergent BioSolutions is the manufacturer of the majority of naloxone being purchased by governments across North America (and beyond) with taxpayers’ money. It does this under the name Adapt Pharma, which is wholly owned by Emergent.
Emergent -- likely not coincidentally -- has a long history of a revolving door between its company, its lobbyists and government. It harnesses that, together with other approaches such as aggressive tactics to sideline competitors, to obtain large numbers of very lucrative contracts for which they are often the only company asked to bid.
Emergent completely dominates government contracts for
nasal-spray naloxone (under the brand name Narcan). (You can see for yourself by searching the
US federal contract-award database for ‘naloxone’ and looking at the name of the company that won the contract.) Most if not all of the contracts are listed as going to Adapt Pharma – which is a
wholly-owned and privately held subsidiary of Emergent. [Unfortunately, a search for ‘naloxone’ in the
Canadian federal government’s ‘Open Government’ contract-award webpage yields only two results and each of those two contracts is for less than $30,000; it clearly is not nearly as comprehensive as the US database.])
And already back in
January 2016 Emergent/Adapt struck a deal to supply its naloxone to 62,000 state and local-government agencies, as well as non-profit organizations. And the wording of the news release suggests this isn't the first such widespread purchasing of naloxone by public bodies.
Notably, Emergent has also sold billions of dollars’ worth of an outdated anthrax vaccine to the US government over several years, in the very unlikely event of a terrorist anthrax attack. (The doses of vaccine are not used, expire after a short period and are replaced with new doses.)
There are several articles detailing the tight bonds between Emergent and key government decision-makers that resulted in these large anthrax-vaccine purchases. Those include
this May 2020 Washington Post article (titled, ‘Before [the] pandemic, Trump’s stockpile chief put the focus on biodefense. An old client benefited’),
this June 2020 Washington Post article (titled, ‘Before the pandemic, top contractor received billions from government to help prepare the nation for biowarfare) and
this March 2021 New York Times article (titled ‘A Who’s Who of revolving-door influence at Emergent BioSolutions’). (Sorry for the paywalls; I’d post the articles on my website but it’s against the law.)
And as a notable and timely subpoint: Emergent has made billions of doses of Covid vaccines for Johnson & Johnson and AstraZeneca at Emergent's Baltimore manufacturing plant. Yet it was revealed in May of this year that because of significant quality-control issues at the plant (which Emergent tried to hide for many months), the ingredients for 400 million doses had to be discarded. See for example
this May 2022 ABC News article. And there’s more: in early August 2022 it was revealed that another approximately 135 million doses of the Johnson & Johnson Covid shot have to be destroyed, also because of quality-control problems. See for example
this CBS News Baltimore piece. As a result, the company temporarily halted manufacture of J&J shots; then it announced on
July 29, 2022, that it will restart production. (Emergent apparently also maintains
it should be paid by J&J for every dose, whether it had to be discarded or not.)
I also found that this pattern is continuing with respect to naloxone/Narcan.
In the US, for example, employees of the top-tier Washington, D.C., lobbying firm
Alpine Group Partners have been working on Emergent’s behalf in D.C. for a few years. (Type ‘naloxone’ into the search box at the top of the
US federal-government lobbying database home page to see this). Some of the
legislation they’ve been pushing includes the ‘
Support, Treatment, And Overdose Prevention [STOP] Fentanyl Act of 2021,’ the ‘
Preventing Overdoses and Saving Lives Act of 2021’ and the ‘
Restoring Hope for Mental Health and Well-Being Act of 2022.’
In Canada most of Emergent’s lobbyists work for
Counsel Public Affairs. You can see for yourself by searching for ‘naloxone’ in the
Canadian federal lobbyist registry, or look at
this search result for ‘naloxone’ in the B.C. lobbyist registry.
Among Emergent’s many well-connected lobbyists is
Seamus Murphy, a partner and federal practice lead in
Counsel Public Affairs. He’s the most frequent federal lobbyist for Emergent/Adapt, starting in 2017. As shown in
this Ottawa Citizen article on the very close ties between lobbyists and the federal Liberal government,
Murphy is married to Leslie Church. Church is chief of staff to Deputy Prime Minister and Finance Minister Chrystia Freeland.
Another is
Jean-Marc Prevost, Counsel’s Vice President, Western Canada, and a former CTV Winnipeg journalist.
The most recent government position Prevost held, immediately before joining Counsel in May 2021, was head British Columbia Health’s communications team under the B.C. Liberal government. Yet another is
Brad Lavigne, a Counsel partner and vice president, Western Canada, and long-time heavy-hitter in the NDP.
2. People who are administered naloxone have been reported to sometimes have severe consequences such as heart attacks, strokes and death.
Thanks no doubt in large part to Emergent’s influence, a huge number of people in very powerful positions are amplifying the message that more naloxone needs to be disseminated. These powerful officials give less weight to measures to stop the overdoses from happening in the first place rather than to relying on naloxone after someone has already overdosed. And they also assert that any potential risks are outweighed by the drug’s ability to quickly reverse a possibly fatal overdose.
The same occurs at every level -- including the vast majority of medical studies on naloxone being skewed to promote rather than objectively examine the widespread dissemination of the medication.
(I contacted Emergent media relations in the U.S. with some questions for this article about the cost and adverse events associated with Narcan.
Assal Hellmer, Emergent’s Senior Director of Business Communications, Global Communications and Public Affairs, got back to me by asking what outlet I’m writing the story for and what my deadline is. I responded, but haven’t heard from her since.)
The World Health Organization appears to believe the same thing; since at least
2002 it has deemed naloxone an ‘
essential medicine.’ These are drugs that are “the most efficacious, safe and cost-effective medicines for priority conditions.”
Yet Emergent’s Canadian product monograph for Narcan itself states that some people have had serious adverse events after receiving the drug. [I couldn’t find a full Narcan product monograph from any other country.]
These include heart attacks, seizures, coma and death.
The Canadian product monograph, which of course is written by Adapt/Emergent, goes on to imply there’s no solid proof naloxone is at fault. For example, it says that, in the case of such events in people who’ve had recent surgery, “pre-existing cardiovascular disorders and/other other drugs may have contributed to the adverse effects. A direct relationship to naloxone has not been established.” And for people who’ve had convulsions or seizures after receiving naloxone, it states, “the relationship between naloxone and convulsion or seizure is unclear.”
Other adverse people have experienced after being given naloxone, according to the product monograph, include racing heart beat (tachycardia), life-threatening abnormal heart rhythm (ventricular fibrillation) and brain damage/brain dysfunction (encephalopathy).
The product monograph also states, among other things, that “T
here are no adequate and well-controlled studies in pregnant women... [
N]aloxone should be used during pregnancy only if clearly needed.” [Bolding added by me.]
This section of the product monograph further notes that, “
It is not known whether [the drug] is excreted in human milk” from breast-feeding women who have been given the drug. The
narcannasalspray.ca website states -- in the Frequently Asked Questions section, under the question, ‘Can Narcan Nasal Spray be used in pregnant women?’ -- that
Narcan may cause preterm labour or be life-threatening to the fetus. [Bolding added by me.]
And what about the interaction of naloxone with other drugs, herbs or food?
Such interactions “have not been established,” the document intones. It’s not clear whether that means any and all potentially negative interactions have not been investigated or that there’s no solid proof that any exist.
I reached out to Health Canada media relations to ask some questions about these serious adverse events.
Andrea Richer responded. She defended the product in her emailed response, using similar language to the Adapt/Emergent product monograph.
Richer wrote, in part:
“While cardiovascular side effects can be serious, the NARCAN product monograph also indicates that these adverse events may be confounded by the effects of other drugs, pre-existing cardiovascular disorders, or related post-operative issues, and that a direct relationship between these adverse events and naloxone has not been established.”
3. Accidental opioid-overdose death tallies likely are highly inflated
Dirk Huyer has been the chief coroner for Ontario, the most populous province in Canada, since 2014. And in that role, he’s the most influential coroner in Canada -- including when it comes to touting the rising tally of opioid-overdose deaths.
For example, last week he apparently showed one journalist, Liam Casey of the Canadian Press, preliminary data on the tally of opioid-overdose deaths in Ontario between April 2021 to March 2022. (There is
no news release about the data from the Ministry of the Solicitor General, the department the chief coroner is part of.) Casey’s article on the data was reposted by most major Canadian news outlets, from the
CBC to
CP24, and from the
Le Devoir to the
Vancouver Sun.
Huyer reportedly told Casey there were 2,790 such deaths in that period. This number is a little higher, according to Huyer, than the 2,727 opioid-related deaths in the April 2020 to March 2021 period, but much higher than between April 2019 and March 2020.
“It’s ongoing and it’s bad and it got heck of a lot worse during the pandemic,” Huyer was quoted by Casey as saying about these new opioid-overdose-death numbers.
“Should we be celebrating the fact that we’ve gone down 10 per cent [compared to the April 2020 to March 2021 period]?” continues Huyer's quote in the article. “No. We still have a lot of people dying, but, yes, we’re not continuing to go up, so that is good.”
But is Huyer giving a true picture of the tally of opioid-overdose deaths, the lion’s share of which he and other officials deem to have been accidental? And is there any solid indication that tallies given by officials from other jurisdictions are any more accurate?
Here are my four reasons for believing the answer to these questions is a resounding ‘No’:
3A. I’ve written several articles uncovering misdeeds on Huyer’s part – for example, his role in making it much harder to determine the true causes of deaths of people in long-term-care homes, and in stonewalling inquiries into other deaths despite years of pleas from the loved ones of the deceased individuals. My articles are
here,
here,
here and
here. (A
Toronto Star columnist mentioned my journalism about Huyer in
her May 2020 article pointing to some questions about him.)
Other journalists have also written about problems surrounding Huyer and his colleague Michael Pollanen, who is Ontario’s chief forensic pathologist. These journalists document that the pair closed the forensic-pathology centre in Hamilton, Ontario, likely in retribution for some of the main pathologists at that Hamilton centre complaining to the province’s coroners’ governing body about Huyer and Pollanen interfering in their death investigations.
Ontario’s auditor general’s team also investigated the province’s Office of the Chief Coroner and Ontario Forensic Pathology Service. She released the results in a section of her
2019 annual report.
There are many remarkable and alarming findings. For example, the second page of the section of that annual report on the Office states:
“Overall, our audit found that the Office does not have effective processes to demonstrate that its coroners and pathologists consistently conduct high-quality death investigations, and does not sufficiently analyze data or follow up on the implementation of its recommendations to improve public safety to help prevent further deaths.
3B. Tallies of the total number of people who died of a particular cause come from the collation of data in thousands or millions of medical certificates of death. Yet it’s well-known in the medical community that there are very high rates of errors and inaccuracy in individual death certificates and even higher rates in the collated data. As just four examples, read
this paper,
this paper,
this one and
this one.
Those papers, among many others, also suggest that officials must have long know about the scope of the problems but have done very little to rectify the situation.
Nor do the officials admit, when trumpeting statistics such as the opioid-overdose tallies, that they are not reliable.
3C. In death certificates of people who had opioids in their bodies when they passed away, the opioids are only allowed to be slotted into six categories in the information entered in the people’s death certificates.
That results -- thanks also to the current political/media emphasis on fentanyl overdose deaths -- in certain types of opioids, primarily fentanyl, being significantly over-represented in death certificates and other drugs being under-represented. (Naloxone only reverses overdoses of opioids, not of other substances such as benzodiazepines and alcohol.)
The overall categorization of causes of death is brought to us by the World Health Organization (WHO) and is formally known as International Statistical Classification of Diseases and Related Health Problems (shortened as ICD) codes.
Of the mere six ICD codes that cover opioids, the first (T40.0) is for opium alone. The second (T40.1) is for heroin alone. The third (T40.2) covers ‘other natural and semisynthetic opioids, including morphine, codeine, oxycodone, hydrocodone, hydromorphone, and oxymorphone.’ The fourth (T40.3) is for methadone.
The fifth (T40.4) covers a number of different ‘synthetic’ opioids – that is, ones that are 'illicitly manufactured.' These include fentanyl, along with several others such as buprenorphine and tramadol.
(The final code (T40.6) is ‘other and unspecified narcotics.’)
(Note that the newest version of the ICD codes list, ICD-11, released in February 2022, and perhaps not yet widely in use, does to my layperson’s eye appear to perhaps rectify a bit of this. There is, for example, a specific code for ‘fentanyl overdose undetermined intent’ (code PH40) and another for ‘intoxication due to multiple specified psychoactive substances (6C4F.3). You can see this by going to the
ICD-11 Coding Tool website, typing ‘fentanyl’ into the search bar at the top and pressing the ‘Enter’ key on your keyboard.)
A
paper published in 2021 documented this (linked also to in point 3B above - it's the third paper in the sentence with four papers hyperlinked to in a row). Among other conclusions in this important paper, the authors wrote that:
“In drug overdose death cases, significant epidemiologic information is lost when each drug mentioned in the death certificate finds its way into a specific ICD T-code category. Presumably, this enables CDC [US Centers for Disease Control and Prevention] officials to be able to state a percentage of drug overdose deaths each year in which, for example, T40.2 or T42.4 drugs were involved. However,
aggregating data like this obscures not only the prevalence of specific drugs in causing overdose deaths, but also ignores entirely the real cause of most fatal overdoses, namely, the additive or toxic interactive effects of polysubstance abuse.” [Bolding added by me.]
3D. And the obfuscation goes even further. The current
Ontario handbook for physicians and coroners on medical certification of death is the only detailed death-certification guide I could find for medical professionals in Canada, the US or elsewhere. The Ontario handbook states:
“
Under current WHO coding rules, deaths due to an external cause that are unspecified as to whether accident, suicide, homicide or of undetermined intent (e.g., the [relevant] section was not completed) are classified as accident until further information is provided.” (Underlining in the original; bolding added by me.)
This appears to be true. I found a website on instructions for ICD-10 coding in the US, including
this webpage on codes for deaths involving drugs such as opioids and chemicals. The webpage states, in the subsection on poisoning: “If the intent of the poisoning is unknown or unspecified, code the intent as accidental intent. The undetermined intent is only for use if the documentation in the record specifies that the intent cannot be determined.”
There are other strong indications that coroners – and all the more so the chief coroner -- are allowed to have a heavy hand in determining what's appropriate to include in death certificates. However, I don’t have room to include them all in this article.
One of the overall results is that virtually all deaths in which an opioid was found in the deceased’s person’s body are categorized as accidents.
But why aren’t deaths of undetermined/uncertain cause simply categorized as such, rather than all of them being automatically put into the ‘accident’ category?
And isn’t it highly plausible that many of the people who are counted as having died accidentally (or as undetermined) from an opioid overdose in fact deliberately killed themselves?
That seems particularly likely to be the case over the last two years when many of us had suicidal thoughts in that dark period of lockdowns, job losses, economic hardship and severe restrictions on our freedoms. But that’s not something governments are eager to admit.
Not to mention that homicides via opioids can be difficult to detect.
Additionally, the rush and frequently not-thorough manner in which death certificates are frequently filled in -- including rarely waiting for ‘further information’ to come in before they’re completed -- as documented in the papers on inaccuracies in death certificates, may well keep the true causes of many deaths from coming to light.
4. There’s a financial incentive for pharmacists, and others, to distribute a lot of naloxone and to perhaps in some cases to skirt the rules in doing so.
Pharmacists in many jurisdictions are reimbursed by the government for the cost of each naloxone kit including a mark-up, and also receive a fee for training people and for dispensing the kits to them. That can add up pretty quickly.
For example, reading this
March 2018 Ontario provincial government document on reimbursement to pharmacists for naloxone kits is revealing.
It states that pharmacists are reimbursed $10 for the dispensing fee for one or two nasal-spray kits per customer, plus $110 for the drug cost plus a mark-up.
The total reimbursement for injectable naloxone kits is $70 – that is, $35 for the kit, a $10 dispensing fee and $25 training fee.
Furthermore, as far as i could determine, there doesn’t appear to be any frequently used mechanism for governments or regulatory bodies to verify how many naloxone kits are sold at any given pharmacy, whether the intranasal or intramuscular form was dispensed – if either -- and whether the required training was given.
Therefore it’s not surprising that Newman isn’t the only person in Ontario who’s been skirting the rules for dispensing naloxone. A search on the Ontario College of Pharmacists’ website shows there have been others
(Robert Awad,
Anna Johannesson and
Kinfe Blad). This is certain also to be occurring in most if not all other jurisdictions.
Also community organizations and some of the other tens of thousands of groups and government departments that distribute naloxone kits may well have similar problematic people among them.
5. Drawbacks of widespread naloxone dissemination -- including solid evidence that broad and indiscriminate access to naloxone does more harm than good -- occasionally come to the general public’s attention. However, that information quickly disappears from view under a wall of silence and/or criticism and denial.
One person pointing to potential drawback was Kelvin Goertzen. This was in a news article from
May 2017, when he was Manitoba’s Minister of Health (Goertzen later became premier of the province).
He expressed concern after hearing that people were using naloxone immediately after taking opioids, in order to keep getting high time and again without risking an overdose.
Goertzen is quoted in that 2017 article as saying the expansion of access to naloxone under his watch had “
been helpful in some ways, but I also don’t want to send the message that naloxone is any way a cure-all because it’s not. Nor should it be relied on in feeding an addiction.” [Bolding added by me.]
(I found other reports of this misuse of naloxone – for example
this one, which was scrubbed from its original place on a media website but I found via archive.org.)
I also discovered a long and impressive research paper that investigated whether or not expanding access to naloxone to very large numbers of the general public has reduced or increased opioid abuse, opioid-related mortality and opioid-related crime. It was written by two American economics/business academics and was
posted online in September 2021 (it’s also listed on the website of one of those academics,
Jennifer Doleac, along with links to the extensive media coverage of it -- scroll down to see her mention of the paper and the coverage it received).
The pair found that
wider naloxone access is associated with increased and/or riskier opioid use (the same concern Goertzen expressed) -- as shown by increased rates of opioid-related emergency-room visits and opioid-related theft – and with no reduction in opioid-related deaths.
The two academics were immediately and vociferously attacked for this paper – see for example
this Forbes piece that includes some of that criticism. But I read the paper and found it to be largely thorough, careful and solid. And the authors were careful in how they worded their findings.
“We emphasize strongly that our findings do not imply that we should limit naloxone availability to individuals suffering from opioid addiction, or those who are at risk of overdose; naloxone has been available through prescription for a long time to these groups, and serves an important role in reducing the risk of opioid overdose deaths,” Doleac and Mukherjee conclude. “
Instead, we should try to find ways to mitigate possible unintended consequences.” [Bolding added by me.]
I’ve put a lot of information together for you, the reader, to ponder. And it’s only part of the mountain of material I’ve sifted through in the last few weeks.
There may be some important some points I’ve missed or errors I’ve made, despite my best efforts. If you know of any, please let me know.
In any case, I hope this articles give you a new perspective on the frequent headlines about growing tallies of opioid-overdose deaths, and the supposed necessity of putting naloxone into the hands of tens of millions of people in North America alone.





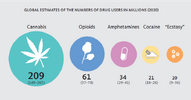
 roll, the Carbon footprints of drug production:
roll, the Carbon footprints of drug production: